

Non pigmented melanocytic nevus of the oral cavity. A case report
Porrini R. 1, Cannas M. 2, Valente G.3, Rocchetti V. 4, Colombo E.5, Sabbatini M.2
1 Private practitioner
2 Research Center of Biocompatibility and Tissue Engineering, Dep. Clinical and Experimental Medicine. Università del Piemonte Orientale “A. Avogadro”, Alessandria, Novara, Vercelli; Italy.
3 Lab. Of Human Pathology, Dep. Clinical and Experimental Medicine. Università del Piemonte Orientale “A. Avogadro”, Alessandria, Novara, Vercelli; Italy.
4 Odontostomatologic Clinic, Dep. Clinical and Experimental Medicine. Università del Piemonte Orientale “A. Avogadro”, Alessandria, Novara, Vercelli; Italy.
5 Dermatology Clinic, Dep. Clinical and Experimental Medicine. Università del Piemonte Orientale “A. Avogadro”, Alessandria, Novara, Vercelli; Italy.
Corrisponding Author:
Maurizio SABBATINI
Research Center of Biocompatibility and Tissue Engineering, Dep. Clinical and Experimental Medicine. Università del Piemonte Orientale “A. Avogadro”,
via Solaroli 17, 28100; Novara
Italy.
Phone : +39 – 0321 - 660634
Fax : +39 – 0321 - 660632
e-mail : maurizio.sabbatini@med.unipmn.it
SUMMARY
We report a case of a 37-year-old caucasian female presenting a 1 cm pinkish nodular asymptomatic lesion of the hard palate, slowly growing in the last years. A diagnosis of non pigmented melanocytic nevus was formulated by means of an oral biopsy. Because of its rarity and to avoid any risk of malignant transformation, a surgical treatment with wide excision was chosen; the surgical wound was previously covered with a membrane of fibrin and autologous platelets, and subsequently sutured, resulting in a total heal. This procedure seems to be the most reliable to approach melanocytic lesions of the oral cavity.
KEY WORDS: oral nevus; non pigmented melanocytic nevus; oral biopsy; oral surgery
INTRODUCTION
Nevi are localized lesions of disembryogenetic origin, congenital or late-manifesting, which derive from one or more components of the skin or of the mucosa (epithelium, stroma, glands capillary vessels)8. They exist as extremely diversified forms, such as rounded, linear, zonal, figured, metameric and multiple nevi10. Sometimes, nevi can also be part of complex malformative syndromes that involve other organs apart from the skin (Von Recklinghausen syndrome, tuberous sclerosis, systemic angiomatoses)8. Thus in dermatopathologic area the term “nevus” is extensively used and encompasses both melanocytic and non-melanocytic lesions.
Melanocytes represent cell deputed to synthesize melanin that is then transferred to the epithelial cells, as well as to macrophages (melanophages). The color of mucosal pigmentation can vary from brown to blue to black depending on the depth of the pigment within the mucosa (Tyndall effect). Therefore from an histological point of view, cutaneous melanocytic nevi are characterized by pure melanocytic hyperplasia or by melanocytic nests at the dermo-epidermal junction (such as junctional nevus), or by nests and cords of melanocytic cells in the upper derma (such as intradermal nevus). Finally, compound nevi are characterized by features of both junctional and intradermal nevi. A similar distinction can be used also for melanocytic lesions of the oral mucosa. In fact, in the basal cell layer of the oral mucosa, melanocytes can be observed similar to those find in the skin.
Nevi can display different intensities of pigmentation (hyperchromic nevi). In some cases, however, nevus cells do not synthesize melanin, or their melanosomes gather in a perinuclear location instead of throughout the cytoplasm; in this case, the lesion and the surrounding skin or mucosa show a similar colour (amelanotic nevus). In particular the amelanotic nevus of the oral mucosa is pinkish, and falls within the category of the so-called “pink lesions”, which offer several problems of differential diagnosis6.
In the present work we deal with clinical presentation of achromic (non pigmented) melanocytic nevus case located to hard palate mucosa.
Case report
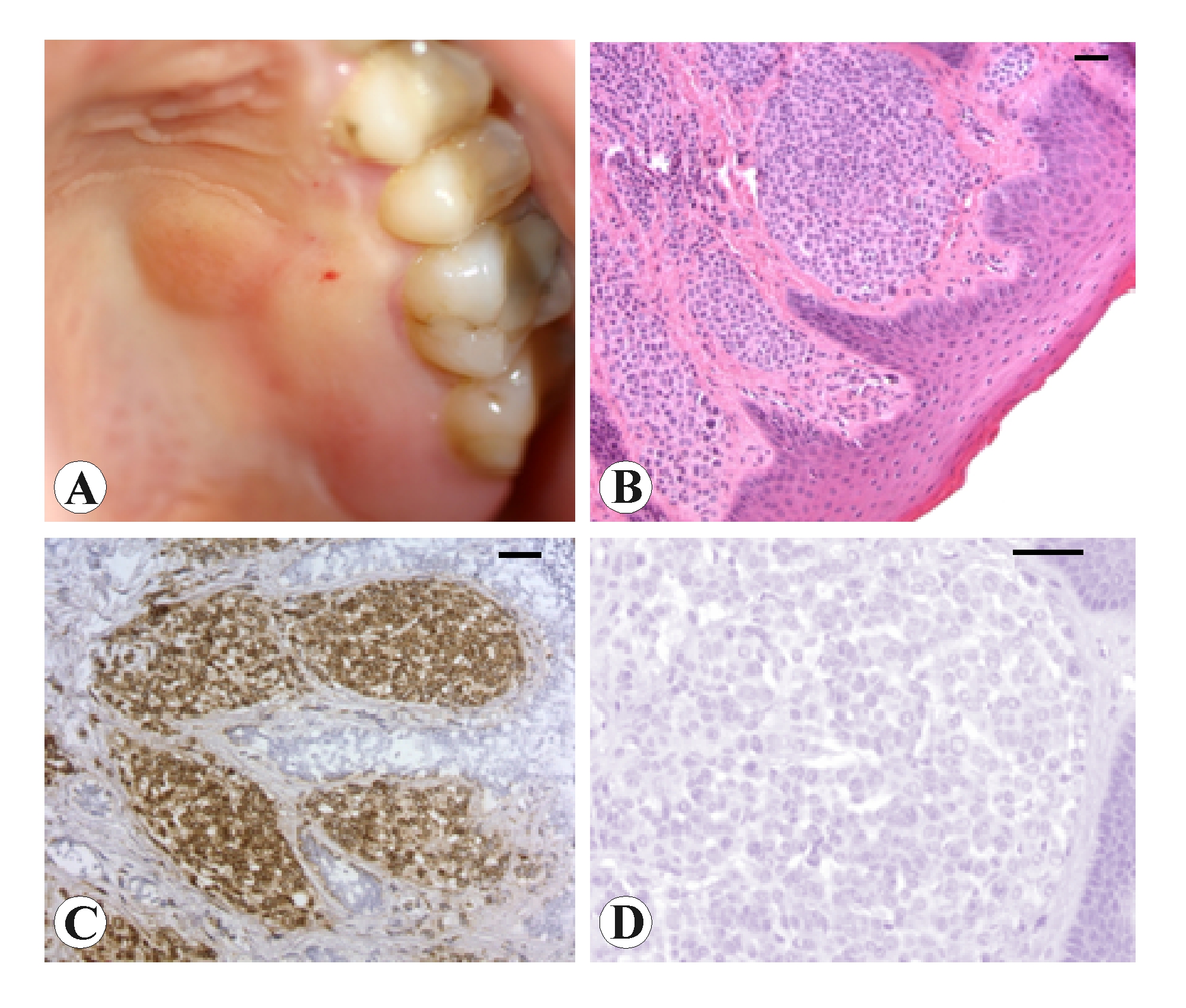
A 37-year-old female patient was referred for routine conservative dentistry therapy. Examination of the oral cavity allowed to detect a roundish lesion slightly protruding. It was a pinkish, painless and firm nodule situated in the molar region of the left hard palate, 1 centimetre in diameter, raised above the surface by approximately 0.5 cm (Fig. 1A). The patient reported that an asymptomatic papule was present 15 years ago, it was growing in the course of the last year, with any subjective symptomatology.
The lesion underwent to excisional biopsy. Histological analysis showed the nevus tissue layered under a continuous squamous epithelium. The stroma contained nests of medium-sized round cells, with regular monomorphous nuclei (Fig. 1B). The nevus cells were immunohistochemically positive for S-100 protein (Fig. 1C), while melanin, visualized by Masson-Fontana silver staining, was absent (Fig. 1D). Following these findings, we formulated diagnosis of achromic intramucous nevus of oral cavity.
Surgery
The patient underwent total excision of the nevus in local anaesthesia. The resection of the lesion was conducted at 3 mm from the borders performing a roundish 1.6-cm loss of tissue in the hard palate (Fig. 2A). Because of the difficulty to make an immediate suture in the palate, we have planned an autologous graft of platelet-enriched fibrin (PRF) to facilitate the formation of granulation tissue3.
Briefly, a few minutes before the operation, 5 ml of the patient’s peripheral venous blood were drowed and placed in a centrifuge (2700 rpm for 12 minutes) to separate the PRF fraction. This was removed from the test tube using sterile forceps (Fig. 2B), and spread on a sterile gauze, previously soaked in physiological solution with metronidazole, to form a thin membrane. Subsequently, the lesion was resected, and the surgical wound was covered with a PRF membrane (Fig. 2C) fixed by absorbable thread (Fig. 2D). A compression was applied for 1h 30 min with swabs of sterile gauze soaked in physiological solution. The patient remained under observation for 3 h, and was discharged with a semi-liquid, cold diet. After seven days, the stitches were removed, showing an advanced healing (Fig. 2E). A subsequent check-up at 28 days revealed a complete recovery of the palatal mucosa (Fig. 2F).
Discussion
Buchner and Hansen2 have reported that, amongst 191 nevi of the oral cavity, the most frequent are intramucous (55%), and that they are located in the hard palate in 23% of the cases. Moreover, 13% of the cases encompassed in this series are not pigmented2. However, this percentage may be overestimated if only clinical findings are considered, since some clinically hyperchromic nevi are histologically amelanotic1. Nevi of oral cavity, independently from their histological appearance, may occur as hypochromic nevi, but the complete lack of melanin is a very rare occurrence, both clinically and histologically5,7. The case we report is rather unusual and pure amelanotic nevi of the oral cavity.
Clinical diagnosis of non-pigmented nevi, either flat and protruding, is difficult, because the nevus shows a pinkish colour that is indistinguishable from that of the surrounding mucosa. Moreover, the localization inside the oral cavity does not allow to use instrumental diagnostic such as dermoscopy4. Many other lesions should be considered in the differential diagnosis, and only histological diagnosis results to be conclusive, to discriminate from a lot of other non pigmented papular and/or nodular lesions6. For this reason, clinical diagnosis was doubtful and only histological assessment was definitely conclusive.
Although nevi of oral cavity are not associated to a higher malignant transformation incidence than similar cutaneous lesions9,10, they should be carefully followed up, mainly in their size increasing , asymmetry and alterations of shape and colour during time. When one of these changes occurs, the lesion should be radically excised, with a wide disease-free margin.
The case presented in this work had not performed shape and colour change, but the lesion had showed a quite rapid growth and it was subjected to a continuous friction during mastication owing its location. Therefore to avoid a potential malignant transformation a wide margins resection was planned.
The surgical excision was repaired by procedure that take in account that palatal mucosa is devoid of a true submucosa and consequently does not allows to perform a correct suture. Therefore to improve and accelerate the healing course and decrease the risk of bleeding, PRF membrane was applied. A shortening of healing time was obtained (6 days) by this method. In particular this technique is widely recommended in the resection of oral lesions, when patients need of a rapid surgery or when an immediate suture is not practicable for anatomical or clinical reasons3.
BIBLIOGRAFIA
- Bhawan J, Cao SL. Amelanotic blue nevus: a variant of blue nevus. Am J Dermatopathol 1999: 21: 225-228.
- Buchner A, Hansen LS. Pigmented nevi of the oral mucosa: a clinicopathologic study of 36 new cases and review of 155 cases from the literature. Part II: Analysis of 191 cases. Oral Surg Oral Med Oral Pathol 1987: 63: 676-682.
- Choukroun J, Diss A, Simonpieri A, Girard MO, Schoeffler C, Dhoan SL, Dohan AJ, Mouhyi J, Dohan DM. Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part IV: clinical effects on tissue healing. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006; 101: e56-e60.
- De Giorgi V, Massi D, Carli P. Dermoscopy in the management of pigmented lesions of the oral mucosa. Oral Oncol 2003: 39: 534-535.
- Gutmann J, Cifuentes C, Gandulfo P, Guesalaga F. Intradermal nevus associated with epidermoid cyst in the mucous membrane of the cheek. Oral Surg Oral Med Oral Pathol 1978: 45: 76-82.
- Johr RH. Pink lesions. Clin Dermatol 2002: 20: 289-296.
- Laskaris G, Kittas C, Triantafyllou A. Unpigmented intramucosal nevus of palate. An unusual clinical presentation. Int J Oral Maxillofac Surg 1994: 23: 39-40.
- Leigheb G. Nevi o nei. Testo Atlante di Dermatologia. Pavia: EDIMES Edizioni Internazionali, 2004.
- Meleti M, Mooi WJ, Casparie MK, van der Waal I. Melanocytic nevi of the oral mucosa - no evidence of increased risk for oral malignant melanoma: an analysis of 119 cases. Oral Oncol 2007: 43 : 976-981.
- Patrick RJ, Fenske NA, Messina JL. Primary mucosal melanoma. J Am Acad Dermatol 2007: 56: 828-834.
LEGENDS TO FIGURES
Fig. 1. Microphotograph panel showing the location of non-pigmented melanocytic nevus (A). Results of biopsy investigation: (B) microanatomical appearance of the nevus; (C) positive reaction to S-100 immunohistochemistry; (D) negative reaction to melanin analysis by Masson-Fontana silver staining. Calibration bar = 100 mm
Fig. 2. Microphotograph panel showing several steps to perform surgical removal of the nevus and PRF healing of palatal mucosa (for details see the text).

Dentista Sicilia, Siracusa
Vedi la scheda
Dentista Lazio, Latina
Vedi la scheda
Dentista Calabria, Cosenza
Vedi la scheda
Dentista Marche, Fermo
Vedi la scheda
Dentista Toscana, Firenze
Vedi la scheda